- EA法は痔核切除とジオン注射を組み合わせた術式(下図)で,国内における痔核(いぼ痔)の標準的手術です.当院でのEA法の5年累積無再発率(5年間再発しない確率)は92.5%,10年累積無再発率は67.2%です.手術後の合併症は3.5%の症例に認められています(発熱1.7%,出血0.9%,肛門周囲膿瘍0.4%など).
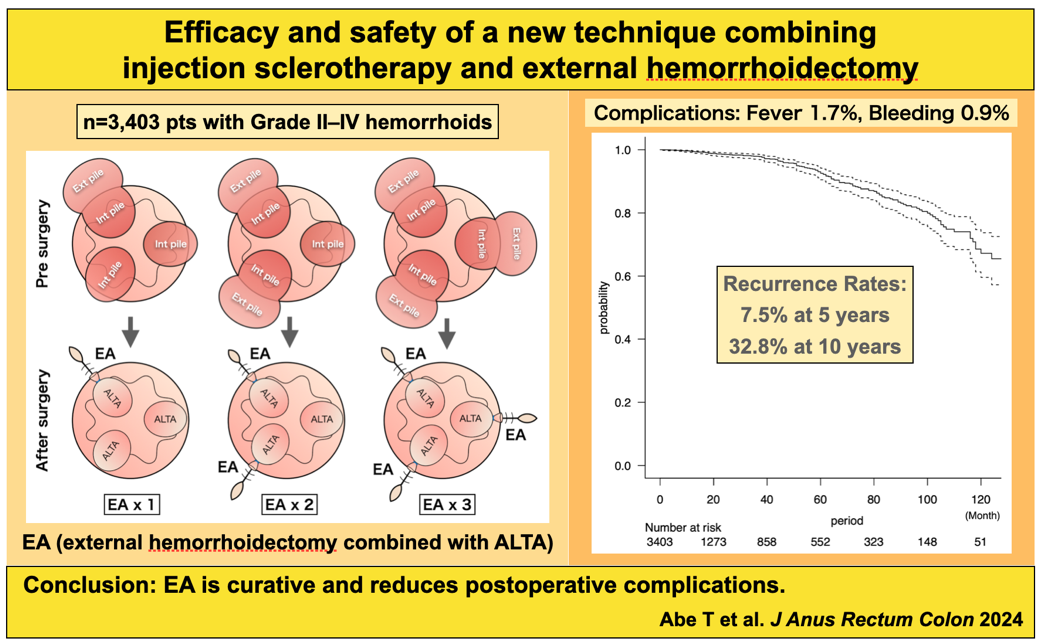
Abe T, Kunimoto M, Hachiro Y, et al. J Anus Rectum Colon 8: 331–339, 2024.
- ALTA単独療法(切らずに治すジオン注射療法)の3年累積無再発率は92.6%,6年累積無再発率は72.8%です.手術後の合併症は3.0%の症例に認められています(発熱1.4%,直腸潰瘍0.9%,直腸狭窄0.4%,肛門周囲膿瘍0.3%).
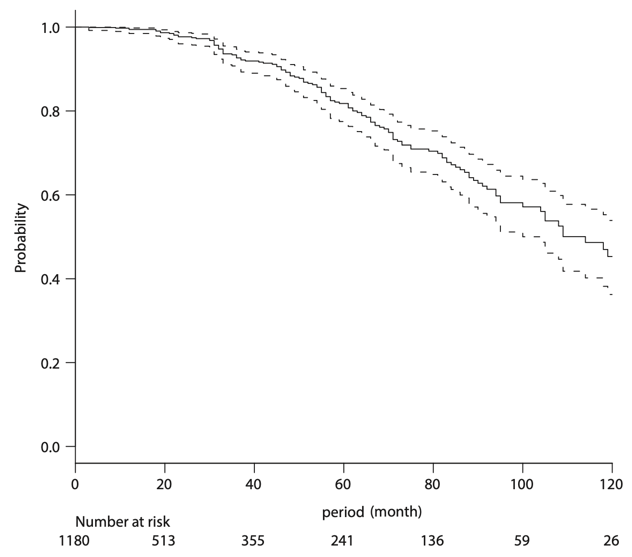
FIGURE. Kaplan-Meier plots indicate the recurrence-free probability for patients after ALTAS. Cumulative recurrence rates at 3, 6, and 9 years were 7.4%, 27.2%, and 47.5%.
Abe T, Kunimoto M, Hachiro Y, et al. Dis Colon Rectum 65(2): 271–5, 2022.
- 用手肛門拡張術は裂肛(切れ痔)に対する当院の標準的手術です.3年累積無再発率は87.9%,5年累積無再発率は69.2%です.術後合併症の発生頻度は2.1%です(血栓性外痔核1.3%,肛門皮垂の腫れ0.8%).
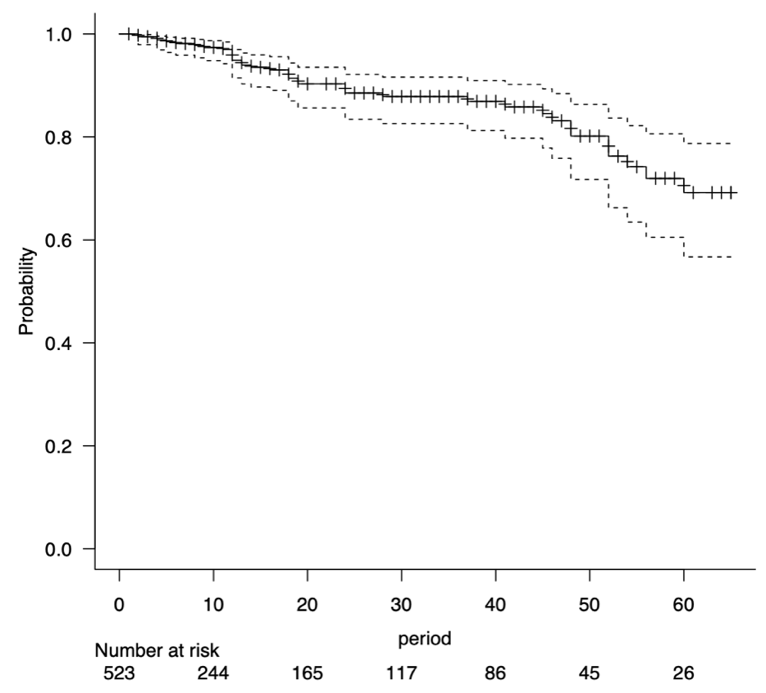
Figure. Probability of no recurrence with time for patients who underwent the treatment (n = 523). Cumulative recurrence- free rates at three and five years postoperatively were 87.9% and 69.2%, respectively.
Abe T, Kunimoto M, Hachiro Y, et al. J Anus Rectum Colon 7: 250–7, 2023.
- 開放式瘻管切除+括約筋固定術は痔瘻に対する当院の標準的手術です.再発率は3%,治癒遷延(治りが遅い)率は1.5%です.一般に痔瘻の手術は便失禁のリスクを伴いますが,当院では図のように肛門括約筋を形成することによって,肛門機能が悪化するのを防いでいます.
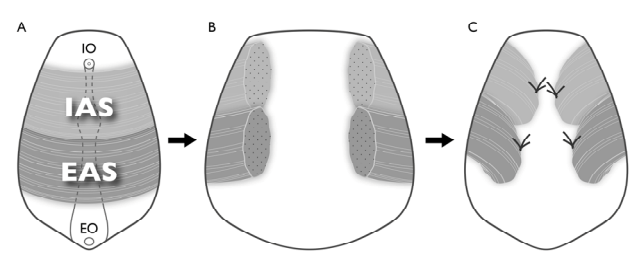
Figure. Detail of open fistulectomy with sphincter fixation. (A) IO = internal opening, EO = external opening, IAS = internal anal sphincter, EAS = external anal sphincter; (B) Sphincter division and total fistulectomy; (C) Both edges of the incised IAS and EAS were sutured to the base of the defect area after fistulectomy.
Abe T, Kunimoto M, Hachiro Y, et al. Open Journal of Gastroenterology 3: 223–6, 2013.
- ALTA硬化療法+肛門縫縮術は高齢者の直腸脱に対する当院の標準的手術です.3年累積無再発率は78.7%,5年累積無再発率は61.4%です.術後合併症の発生頻度は25.5%で,一時的な排便困難(11.3%),創部の感染(8.4%),補綴材の露出(2.8%)などが主な合併症です.
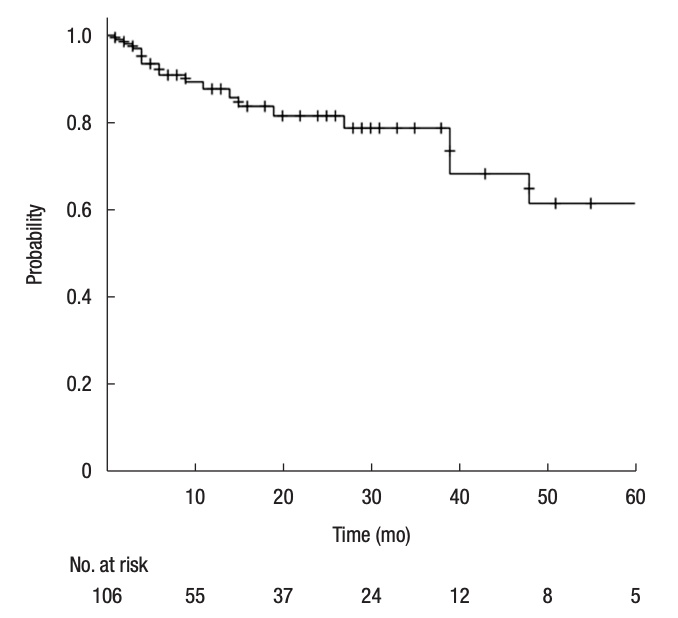
Figure. Probability of no recurrence with time for patients who underwent the treatment. Cumulative recurrence-free rates at 3 and 5 years postoperatively were 78.7% and 61.4%, respectively.
Abe T, Kunimoto M, Hachiro Y, et al. Ann Coloproctol 39:210-5, 2023.